
A direct care provider working in a group home looks at the clock and sees that it’s 2 p.m. - too late to hand out the medications scheduled for noon. Protocol is to immediately contact a Medication Administration Program (MAP) consultant and the employee will have an official medication occurrence on his or her record.
Many companies contracted to operate group homes for the Department of Developmental Services (DDS) allow three medication errors (or “occurrences”), before an employee is either retrained or fired. When a person is one lost paycheck away from their life falling apart, the prospect of weeks to months of lost paychecks is a nightmare scenario, especially when the job provides health insurance.
So why would a person risk their job risk it when perhaps they could just wait it out, make sure the client who missed the medication, or got the wrong medication doesn’t die or have any obvious adverse reaction, and resolve to never make a med error again. Until they do.
In group homes across Massachusetts, the administration of medication is entrusted not to medical professionals such as nurses, but to direct care providers who pass a three-day course in the MAP.
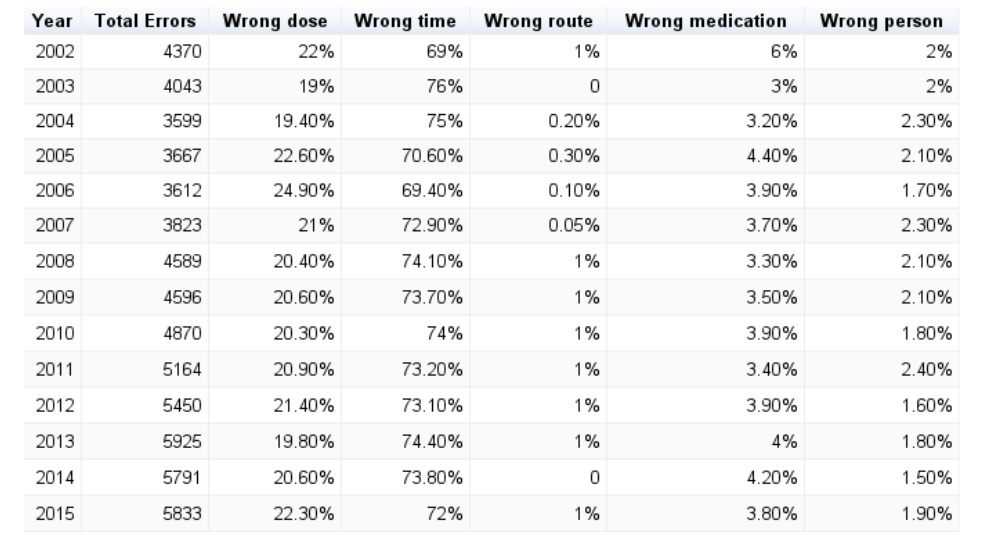
The relatively low number of medication errors that occur each year according to the Massachusetts DDS seems miraculous in light of the limited training and large number of doses handed out every year. DDS estimates that in 2015, there were 5,833 medication errors out of the approximately 41.9 million doses of medication doled out.
Expecting employees who make little more than minimum wage to self report mistakes that could result in the loss of a job that provides regular hours and health insurance is unrealistic. It places employees in an extremely difficult position, which in turn puts DDS clients at risk.
The impact this sort of mistake can have on a client obviously varies depending on the type of medication. For example, a person will have a less severe reaction to missing a dose of an antihistimine than they would to receiving a large dose of antipsychotics that aren’t prescribed to them.
Some companies, for example the May Institute, provide the bare minimum of training in medication administration - 16 hours over three days. One could also look at it as four years worth of nursing school crammed into three days. Hiring a nurse for every residential facility - or even one nurse for every five facilities - would be far more expensive than giving bare bones training to employees making $25,000 to $30,000 per year.
Nurses train direct care staff, and pop in for the occasional surprise visit at residential facilities to see if the med books are in order, the medication closet is locked, and the narcotics are double locked, but they aren’t there every day to distribute medication or to provide their expertise while observing a client’s reaction to medications.
For example, increasing a person’s dose of Prozac can cause stomach problems that make it difficult for a person to eat. The average direct care provider is not nearly as likely to know this as a nurse would be and might misinterpret a client’s refusal to eat as a bid for attention or a sign of depression as opposed to a normal reaction to physical discomfort.
A system of self-reporting will not succeed when employees are set up for failure through a combination of inadequate training, and the fear of making a mistake and losing their jobs. Companies contracted with DDS to run residential facilities relentlessly hammer home the seriousness of medication administration to its employees, but the unwillingness of these companies to hire medical professionals to administer medication belies the fact that they’re shirking their responsibility to provide the best care possible, and in the process, shifting that responsibility to their lowest paid employees.
Read DDS’ full data on medication occurances embedded below, or on the request page.
Image via Pexels




{kind=link}